
Age-related changes of serum tartrate-resistant acid phosphatase 5b and the relationship with bone mineral density in Chinese women1
Introduction
In China, the proportion of aged citizens is growing at an unusually rapid rate. Thus, postmenopausal osteoporosis has been a common disorder that imposes considerable health problems and economic loss. Bone mineral density (BMD) measured by duel-energy X-ray dual-energy absorptiometry (DXA) is the “gold parameter” for the diagnosis of osteopenia and osteoporosis. However, BMD changes rather slowly, and can hardly be detected until substantial bone loss has occurred. BMD provides a static parameter of skeletal status. Therefore bone turnover markers would be useful to have dynamic tests that could identify women at risk before bone loss occurs. For early detection of bone loss, various biochemical markers reflecting bone turnover have been investigated[1,2], and used as an independent factor of BMD to predict osteoporotic fracture risk and evaluate the effect of antiresorptive treatment. In the 1990s, assays were developed to monitor osteoclastic activity by collagen breakdown, such as C-terminal cross-linked telopeptides of type I collagen (CTX), N-terminal cross-linked telopeptides of type I collagen (NTX) and deoxypyridinoline (DPD). However, the above markers are mainly assessed by urinary measurement. The urinary levels of these markers need to be corrected with urinary creatinine concentration because of individual differences in renal clearance. Moreover, serum CTX and NTX levels could be affected by dietary intake.
Recently, tartrate-resistant acid phosphatase5b (TRACP5b) has been used as a potential marker to evaluate the bone resorption rate[3–6]. It is normally secreted by osteoclasts during bone resorption[3,7]. Among several advantages, serum TRACP5b activity has a low diurnal variability, and its level is not affected by feeding, and it does not accumulate into the circulation in renal or hepatic failure, so that the serum samples could be collected at any time of the day. The serum TRACP5b level can be specifically measured by immunoassays and has been proposed as a marker of bone resorption[3–6]. Previous studies in Finland have shown that serum TRACP5b activity determined by immunoassay is a specific and sensitive marker of bone resorption, and TRACP5b activity was significantly elevated in patients with osteoporosis and had a significant negative correlation with BMD[8–10]. More recently, Ohashi et al reported that postmenopausal women had higher TRACP5b concentrations than premenopausal women in Japan[4]. However, due to genetic factors, geographic setting and lifestyle, the pattern of bone turnover could be different among Caucasians, Japanese and Chinese women. In this study, we conducted a cross-sectional study to investigate the age-related change of serum TRACP5b and its correlation with BMD in 722 Chinese mainland women aged 20–79 years.
Experimental subjects
The reference population was randomly recruited from the inhabitants in 6 communities of Shanghai, located on the mid-east coast of China, through a local health organization that is in charge of public health at local community medical stations. Nine-hundred females were randomly recruited and filled out detailed questionnaires. For each study subject, we have surveyed the information on age, sex, medical history, family history, female history, physical activity, alcohol use, dietary habits, smoking history, etc. All of the participants were given a physical examination and screened in order to exclude conditions known to affect bone metabolism, including hyperthyroidism, diabetes mellitus, primary hyperparathyroidism, renal failure, pituitary and adrenal diseases, oligo-menorrhea or amenorrhea before the age of 40. Subjects were also excluded if they were receiving glucocorticoids, antiresorption therapy. As a result, 722 subjects aged 20–79 years were included for the statistical study. In all subjects, 504 were postmenopausal women. The mean age of menopause was 49.3±0.2 years (range 42–56). Two-hundred and eighteen were premenopausal women and had menstrual regularity. The study protocol was approved by the Committee on the Ethics of Human Research of the Sixth People’s Hospital, Shanghai Jiao Tong University.
Materials and methods
TRACP5b immunoassays Blood samples were obtained in the morning after overnight fasting. Serum was separated by centrifugation, aliquoted, and stored at –80°C until the analysis. Serum TRACP5b level was analyzed by a solid-phase, immunofixed, enzyme activity assay as described earlier (SBA Sciences, Turku, Finland)[3]. The interassay analytic error (% CV) was determined by assay of aliquots of 10 sera ranging from to 3.08 U/L to 3.77 U/L on 10 separate occasions; the average CV was calculated to be 7.9%. The intraassay error was determined by simultaneous assay of 6 duplicates of one sera ranging in activity from 2.50 U/L to 3.87 U/L, and the average CV was calculated to be 5.1%.
BMD measurements BMD (g/cm2) of the anteroposterior lumber spine 1–4 (L1–4) and left proximal femur including femoral neck, trochanter, intertrochanter, and total hip was measured by DXA on a Lunar-Prodigy (GE Lunar Corp, Madison, WI, USA). The Lunar device was calibrated daily, and the coefficient of variability (CV) values of the BMD (which were obtained from 10 individuals repeatedly measured 5 times) at L1–4, total hip, femoral neck, trochanter and intertrochanter were 1.39%, 0.70%, 2.22%, 1.41% and 1.19%, respectively. The long-term reproducibility of our DXA instrument during the trial based on weekly repeated phantom measurements was 0.45%. Lumbar BMD was measured from L1 to L4 in the anteroposterior view with fractured vertebrae being excluded from the analysis. According to the World Health Organization (WHO), osteoporosis is defined as BMD more than 2.5 standard deviation (SD) below the mean for young adult women (later clarified as T-score ≤–2.5). Osteopenia is defined as BMD between 1.0 and 2.5 below the mean for young adult women (T-score >–2.5 and <–1.0).
Statistical analysis Individuals were stratified by 10-year age groups, and the results were presented as the mean±SD. The serum TRACP5b concentration change with age and years since menopause were evaluated and the best-fitting model were determined with the highest R2 from a comparison of eight different regression models including linear, logarithmic, quadratic, cubic, compound, power, growth, and exponential equations. Differences between groups were tested using independent samples t-test. The correlations between TRACP5b and BMD at various skeletal sites were determined using Pearson correlation analysis. ANOVA analysis was used to assess the statistical significance of different groups. P<0.05 was considered as statistically significant.
Results
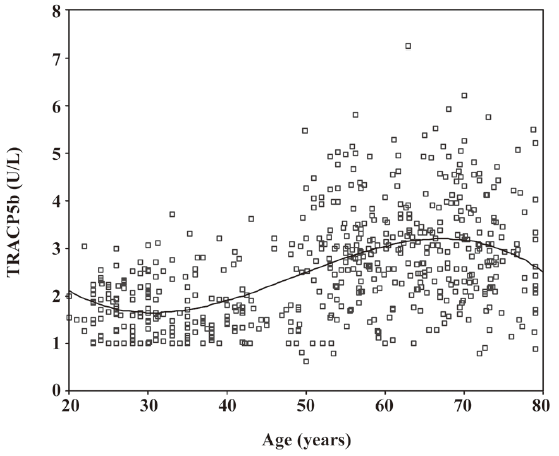
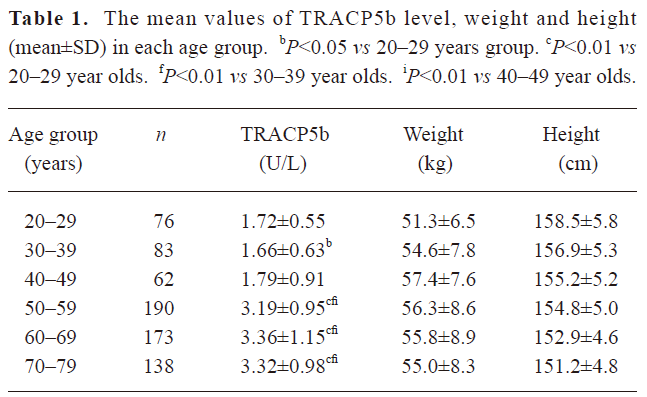
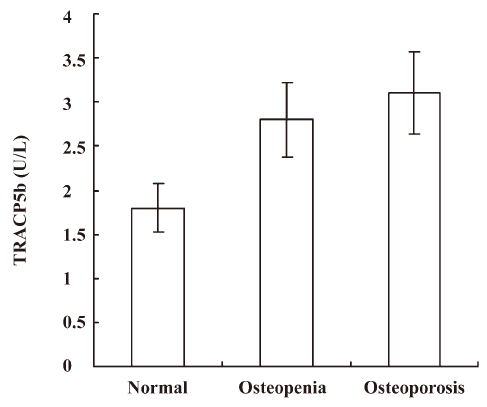
Age-related changes of serum TRACP5b Serum TRACP5b with age-related changes were analyzed using 8 models. All regression models had a fitting effect with coefficients of determinants (R2) indicating a significant difference (P<0.001). However, the cubic polynomial regression model was the best-fitting model for age-related variations of TRACP5b with the greatest value for R2 (R2=0.274) (Figure 1). The levels for the subjects in the age range of 20–29 were slightly higher than those of the subjects aged 30–39. In the subjects aged 30–39, the values reached the minimum level, then it started to increase gradually from the subjects aged 40–49. The TRACP5b level dramatically increased in the subjects aged 50–59, reached a maximum value in the subjects aged 60–69, and then slightly dropped in the subjects aged 70–79 (Table 1). When all subjects were grouped by menopause, the values of TRACP5b were significantly higher in postmenopausal women (3.29±1.07) U/L than in premenopausal ones (1.70±0.59) U/L. In all postmenopausal women, however, there is no significant difference of TRACP5b level, whether these women had menopause for less than 5 years (n=108), between 5–10 years (n=121), or for more than 10 years (n=275) (Figure 2).
Full table
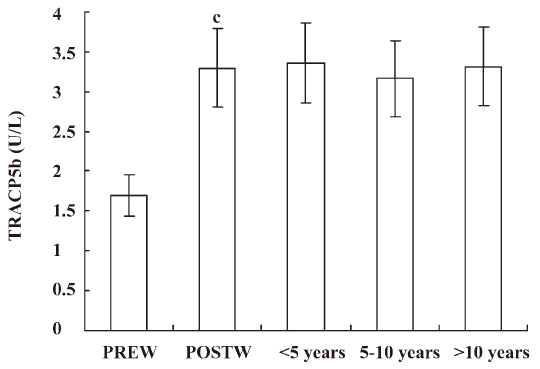
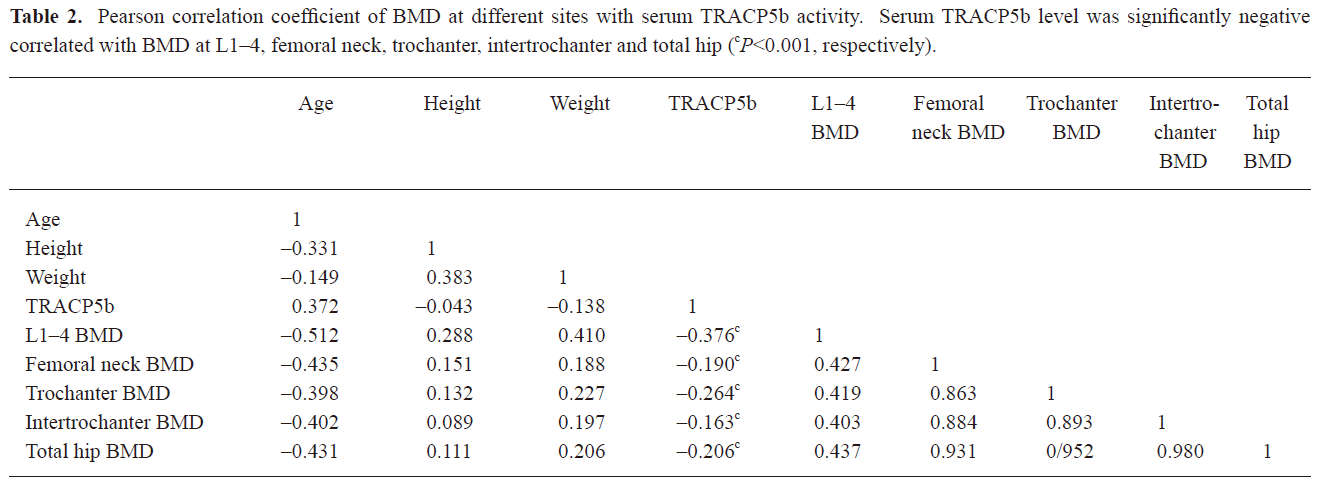
Relationship between serum levels of TRACP5b and BMD When all postmenopausal women were grouped by T-score of BMD, the level of TRACP5b was significantly higher in women with osteoporosis (T≤–2.5, n=268) and osteopenia (T-score <–1 and >–2.5, n=206) than in women with normal bone mass (including premenopausal and postmenopausal women) (P<0.001, n=248). There was also a significant difference of the TRACP5b value between the osteoporotic women and osteopenia women (P<0.05) (Figure 3). The serum TRACP5b level had significantly inverse correlations with BMD at L1–4, total hip, femoral neck, trochanter, and intertrochanter by Pearson’s analysis (P<0.001, respectively), with the decreasing of BMD, the values of TRACP5b increased. The correlation coefficient of TRACP5b level to BMD at L1–4 was higher than that at the femoral neck (Table 2).
Full table
Discussion
Recently, various proteins and enzymes have been used as biochemical markers of bone turnover for the diagnosis of bone metabolic diseases or as indices of therapeutic alternatives[1,211]. Previous studies suggested that bone absorption markers such as CTX, NTX and DPD are higher in postmenopausal women with decreased BMD[12,13]. Unfortunately, the coefficient of variation of some markers (alkaline phosphatase, DPD and urine NTX) was high and was affected by diet and renal clearance. The greater sensitivity of the new bone markers and development of specific, sensitive, and reproducible methods should lead to better diagnostic accuracy in identifying subjects with high bone turnover. TRACP5b is secreted by osteoclasts and has recently been described as a specific and sensitive serum marker of bone resorption[14,15]. TRACP5b appeared to correlate with other markers of bone turnover and BMD[9]. But the age-related changes of serum TRACP5b have not been critically examined in a large Chinese sample in China mainland, although it has been reported in Finland, Japanese and Taiwan region women[4,14–17]. In the present study, we systematically analyzed TRACP5b levels among different age groups of Chinese mainland women. We used a cubic regression model as best fit to analyze age-related variations of serum TRACP5b levels among chosen Chinese females. We found that the levels of TRACP5b significantly increased in Chinese mainland postmenopausal women, the results are consistent with Finish, Japanese and Taiwanese. Furthermore, in our study, we identified that the subjects had the lowest level of TRACP5b in their early 30s, which suggested a correlation with the attainment of peak bone mass around this period. In our previous studies, we found that BMD varied with age and peak bone mass occurred in the age range of 30–35 in Chinese women[18,19]. The levels of serum TRACP5b significantly increased for women aged 50–59, which may be associated with aging and menopause; osteoclastic activity rapidly increase after menopause in women.
In this study, the level of TRACP5b was significantly higher in postmenopausal women with low BMD than that in premenopausal women. The presence of high levels of TRACP5b in postmenopausal women is probably related to an increase in bone resorption. Many studies have indicated that at least a third of all patients with osteoporosis in menopause have a higher bone turnover[20,21], especially in the early first 10 years of the postmenopausal period. We therefore presumed that the level of serum TRACP5b would be higher in the early postmenopausal women than that in the late postmenopausal women. However, there was no significant difference in the levels of serum TRACP5b in women in a postmenopausal period of less than 5 years or 5–10 years compared with those with a postmenopausal period of more than 10 years in this study. Our results were completely in agreement with the findings of a Japanese study. Nishizawa et al[22] reported that serum TRACP5b levels in the postmenopausal women was significantly higher than in the premenopausal women and men, but TRACP5b activity did not increase with years since menopause.
Our study also indicated that a high level of serum TRACP5b was correlated inversely to BMD. TRACP5b significantly increased in postmenopausal women with osteoporosis or osteopenia as compared with women with normal bone mass. The results are consistent with several previous studies where postmenopausal women with high TRACP5b had low BMD and high incidence of bone fracture[18,23,24]. This can be explained by an association of high bone turnover level with a continuous and rapid bone loss in postmenopausal women[25]. Postmenopausal women with a high level of serum TRACP5b were at high risk of having low T-score of BMD, which predicted that the women were undergoing rapid bone loss. Additionally, we found that TRACP5b was a better predictor of BMD in the lumbar spine with mainly cancellous bone compared to the neck with abundant cortical bone. It may be partially explained by the fact that the metabolic turnover rate of cancellous bone is several times higher than that of cortical bone. So, age-related increase of serum TRACP5b suggested that it is a valid clinical strategy for identifying women at high risk for osteoporotic fractures.
In conclusion, serum TRACP5b was a sensitive and useful parameter for the evaluation of age-related changes of bone absorption. High levels of TRACP5b were significantly correlated with low BMD at lumbar spine and proximal femur, and high levels of serum TRACP5b may be a predictor for low BMD T-scores. In the study we have established the reference value of serum TRACP5b in Chinese mainland women. It will be useful in the evaluation of bone turnover status and in monitoring antiosteoporotic agent therapy.
Acknowledgement
We thank 2 anonymous reviewers for comments that improved the manuscript and will aid our future research.
References
- Looker AC, Bauer DC, Chesnut CH 3rd, Gundberg CM, Hochberg MC, Klee G, et al. Clinical use of biochemical markers of bone remodeling: current status and future directions. Osteooros Int 2000;11:467-80.
- De Leo V, Ditto A, la Marca A, Lanzetta D, Massafra C, Morgante G, et al. Bone mineral density and biochemical markers of bone turnover in peri- and postmenopausal women. Calcif Tisue Int 2000;66:263-7.
- Halleen JM, Alatalo SL, Suominen H, Cheng S, Janckila AJ, Väänänen HK. Tartrate-resistant acid phosphatase 5b: a novel serum marker of bone resorption. J Bone Miner Res 2000;15:1337-45.
- Ohashi T, Igarashi Y, Mochizuki Y, Miura T, Inaba N, Katayama K, et al. Development of a novel fragments absorbed immunocapture enzyme assay system for tartrate-resistant acid phosphatase 5b. Clin Chim Acta 2007;376:205-12.
- Halleen JM, Hentunen TA, Karp M, Käkönen SM, Pettersson K, Väänänen HK. Characterization of serum tartrate-resistant acid phosphatase and development of a direct two-site immunoassay. J Bone Miner Res 1998;13:683-7.
- Miyazaki S, Igarashi M, Nagata A, Tominaga Y, Onodera K, Komoda T. Development of immunoassays for type-5 tartrate-resistant aid phosphatase in human serum. Clin Chim Acta 2003;329:109-15.
- Väänänen HK, Zhao H, Mulari M, Halleen JM. The cell biology of osteoclast function. J Cell Sci 2000;113:377-81.
- Rosenbrock H, Seifert-Klauss V, Kaspar S, Busch R, Luppa PB. Changes of biochemical bone markers during the menopausal transition. Clin Chem Lab Med 2002;40:143-51.
- Halleen JM, Ylipahkala H, Alatalo SL, Janckila AJ, Heikkinen JE, Suominen H, et al. Serum tartrate-resistant acid phosphatase 5b, but not 5a, correlates with other markers of bone turnover and bone mineral density. Calcif Tissue Int 2002;71:20-5.
- Halleen HM. Tartrate-resistant acid phosphatase 5b is a specific and sensitive marker of bone resorption. Anticancer Res 2003;23:1027-9.
- Nishizawa Y, Nakamura T, Ohta H, Kushida K, Gorai I, Shiraki M, et al. Guideline for the use of biochemical markers of bone turnover in osteoporosis. J Bone Miner Metab 2005;23:97-104.
- Shan PF, Wu XP, Zhang H, Luo XH, Cao XZ, Xie H, et al. Age-related changes of serum bone alkaline phosphatase and cross-linked C-telopeptides of type I collagen and relationship with bone mineral density in Chinese women. Clin Chim Acta 2006;366:233-8.
- Yan L, Prentice A, Zhou B, Zhang H, Wang X, Stirling DM, et al. Age- and gender-related differences in bone mineral status and biochemical markers of bone metabolism in Northern Chinese men and women. Bone 2002;30:412-5.
- Halleen JM, Alatalo SL, Janckila AJ, Woitge HW, Seibel MJ, Väänänen HK. Serum tartrate-resistant acid phosphatase 5b is a specific and sensitive marker of bone resorption. Clin Chem 2001;47:597-600.
- Miyazaki S, Igarashi M, Nagata A, Tominaga Y, Onodera K, Komoda T. Development of immunoassays for type-5 tartrate-resistant acid phosphatase in human serum. Clin Chim Acta 2003;329:109-15.
- Janckila AJ, Takahashi K, Sun SZ, Yam LT. Tartrate-resistant acid phosphatase isoform 5b as serum marker for osteoclastic activity. Clin Chem 2001;47:74-80.
- Chao TY, Yu JC, Ku CH, Chen MM, Lee SH, Janckila AJ, et al. Tartrate-resistant acid phosphatase 5b is a useful serum marker for extensive bone metastasis in breast cancer patients. Clin Cancer Res 2005;11:544-50.
- Huang QR, Zhou Q, Lu JH, Hu YQ, Liu YJ, Qin YJ. Bone mineral density and age-related bone loss in 2111 healthy women in Shanghai. Chin J Osteoporos 2002;8:191-4.
- Zhang ZL, He JW, Qin YJ, Hu YQ, Li M, Liu YJ, et al. Association between the SNPs and haplotypes in the PPARGC1 and adiponectin genes and bone mineral density in Chinese women and men. Acta Pharmacol Sin 2007;28:287-95.
- Garnero P, Shih WJ, Gineyts E, Karpf DB, Delmas PD. Comparison of new biochemical markers of bone turnover in late postmenopausal osteoporotic women in response to alendronate treatment. J Clin Endocrinol Metab 1994;79:1693-700.
- Garnero P, Grimaux M, Demiaux B, Preaudat C, Seguin P, Delmas PD. Measurement of serum osteocalcin with a human-specific two-site immunoradiometric assay. J Bone Miner Res 1992;7:1389-98.
- Nishizawa Y, Inaba M, Ishii M, Yamashita H, Miki T, Goto H, et al. Reference intervals of serum tartrate-resistant acid phosphatase type 5b activity measured with a novel assay in Japanese subjects. J Bone Miner Metab 2008;26:265-70.
- Gerdhem P, Ivaska KK, Alatalo SL, Halleen JM, Hellman J, Isaksson A, et al. Biochemical marker of bone metabolism and prediction of fracture in elderly women. J Bone Miner Res 2004;19:386-93.
- Välimäki MJ, Tähtelä R. Serum tartrate-resistant acid phosphatase 5b or amino-terminal propeptide of type I procollagen for monitoring bisphosphonate therapy in postmenopausal osteoporosis? Clin Chem 2005;51:2382-5.
- Rogers A, Hannon RA, Eastell R. Biochemical markers as predictors of rates of bone loss after menopause. J Bone Miner Res 2000;15:1398-404.