
Relationship between leukocyte count and angiographical characteristics of coronary atherosclerosis1
Introduction
Inflammation is a key feature of atherosclerosis, and leukocyte count is a marker of inflammation that is widely available in clinical practice. Numerous epidemiological and clinical studies have shown leukocytosis to be an independent predictor of future cardiovascular events, both in healthy individuals free of coronary heart disease, and in patients with stable angina, unstable angina, or a history of myocardial infarction. This relationship has been observed in prospective and retrospective cohort studies, as well as in case-control studies[1]. The relationship is strong, consistent, temporal, dose-dependent, and biologically plausible. Elevated differential cell counts, including eosinophil, neutrophil, and monocyte counts, also predict the future incidence of coronary heart disease[2]. Clinical studies suggest that neutrophil infiltration is actively associated with acute coronary events. The high number of neutral endopeptidase-positive neutrophils in ruptured plaques, compared with eroded plaques, may reflect differences in the underlying pathophysiological mechanisms[3]. However, there is little information available about the association between the angiographical characteristics of coronary atherosclerosis as estimated by conventional coronary angiography and circulating leukocyte count.
Gensini’s scoring system assigns a severity score for a stenosed vessel depending on the degree of luminal narrowing and the importance of its location[4]. Therefore, we evaluated the association between the angiographical characteristics of coronary atherosclerosis and circulating leukocyte count.
Materials and methods
Study subjects The study population consisted of 507 consecutive patients who underwent coronary angiography for suspected or known coronary atherosclerosis at the First Affiliated Hospital of Nanjing Medical University, Nanjing, China, from 2004 to 2005. Patients with spastic angina pectoris (ie, acetylcholine-positive) were excluded. Patients with 2-week infectious processes before catheterization, heart failure (Killip class =2 after acute myocardial infarction), hepatic dysfunction, vascular disease (aortitis treated with prednisolone), familial hypercholesterolemia, thyroid dysfunction, or adrenal dysfunction were also excluded. This study was approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University and informed consent was obtained from all patients.
Coronary angiography Coronary arteries were cannulated by using the Judkins technique[5] with 5F catheters, and recorded on Kodak, 35 mm Cinefilm at a rate of 30 frames per second. When stenotic coronary arteries were found, the presence of stenosis was determined by using a computer-assisted coronary angiography analysis system (Mipron 1; Kontron) after the direct intracoronary injection of isosorbide dinitrate (ISDN; 2.5 mg in 5 mL solution over 20 s). One minute after the injection of ISDN through the Judkins catheter, coronary angiography was performed from several projections. The severity of coronary atherosclerosis was measured by using Gensini’s scoring system, based on the hypothesis that the severity of coronary heart disease is a consequence of the functional significance of vascular narrowing and the extent of the area perfused by the involved vessel or vessels. In this scoring system, a greater reduction of the lumen diameter is assigned a higher score than a distal lesion[4].
Cigarette smoking and alcohol intake The subjects’ cigarette smoking and alcohol intake habbits were assessed by means of a standardized questionnaire. Past or current smokers were asked about the number of cigarettes smoked per day, and those who reported smoking at least 1 cigarette per day during the preceding year were classified as current smokers. With regard to smoking status, subjects were classified as “never a smoker” and “smoker” (including “formerly a smoker” and “currently a smoker”). Subjects who reported consuming at least 50 g alcohol/week were regarded as “current drinkers”. Subjects were classified as “never a drinker” and “drinker” (including “formerly a drinker” and “currently a drinker”).
Anthropometric measurements Anthropometric measurements were taken after the patients had removed their shoes and upper garments and had donned an examining gown. Each measurement was performed twice and the average was used in the analysis. Height was measured to the nearest 0.1 cm using a wall-mounted stadiometer. Weight was measured to the nearest 0.1 kg using a hospital balance beam scale. Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m2). Blood pressure was measured in the right arm with the participant seated and the arm bared. Three readings were recorded for each individual, and the average was recorded.
Hematological measurements Blood samples from every patient were taken at admission to the coronary unit and measurements including total leukocyte count, neutrophil count, eosinophil count, lymphocyte count, monocyte count, basophil count, hemoglobin, erythrocyte count, and platelet count were carried out by an automated blood analyzer.
Laboratory measurements The 12-h fasting blood samples were taken in the morning and the sera were stored at -70 oC immediately after centrifugation until being assayed. All laboratory measurements were conducted at the Central Clinical Laboratory at the First Affiliated Hospital of Nanjing Medical University. Total cholesterol, triglyceride, fasting blood glucose, urea, creatinine, and uric acid were determined by enzymatic procedures on an automated autoanalyzer (AU 2700 Olympus, 1st Chemical Ltd, Japan). The laboratory was monitored for the precision and accuracy of glucose and lipid measurements by the surveillance program. Measurements of agency-assigned quality control samples showed no consistent bias over time within or between surveys.
Statistical analysis Data analysis was performed using the Statistical Package for the Social Sciences (SPSS for Windows, version 10.0; SPSS, Chicago, IL, USA). Patients were classified into 3 groups with low, intermediate, and high Gensini’s scores using the tertile values as cutoff points, so that each group had an approximately equal number of patients to minimize any bias that may have been produced in the statistical analysis. Results for continuous variables are expressed as mean±SD and comparisons of continuous variables were analyzed by the one-way analysis of variance (ANOVA). Categorical variables were compared among the groups of patients by a chi-squared analysis. The Spearman two-way test was used to assess the relationship between 2 quantitative variables. We assessed independent predictors of Gensini’s score with multiple regression analysis. Differences were considered to be significant if the null hypothesis could be rejected with >95% confidence. All P values are 2-tailed.
Results
Clinical and biochemical characteristics in patients grouped according to Gensini’s score Table 1 show the clinical and biochemical characteristics in patients grouped according to Gensini’s score, tertile values of which were used as cutoff points. Patients in tertiles I, II, and III had an increasingly higher Gensini’s score. The frequency distribution of sex (P=0.009) and smoking status (P=0.000) were different among the 3 groups, and drinking status was similar among the 3 groups. The distribution levels of BMI, systolic blood pressure, total cholesterol, triglyceride, uric acid, eosinophil count, basophil count, and lymphocyte count were similar among the 3 groups (P>0.05), whereas those of age (P=0.000), diastolic blood pressure (P=0.011), fasting blood glucose (P=0.000), urea (P=0.012), creatinine (P=0.005), leukocyte count (P=0.000), neutrophil count (P=0.000), monocyte count (P=0.000), hemoglobin (P=0.000), erythrocyte count (P=0.008) and platelet count (P=0.019) differed among the groups.

Full table
Spearman correlations between Gensini’s score and leukocyte count, anthropometric measurements, and biochemical characteristics in patients Table 2 shows the results of Spearman correlations between Gensini’s score and leukocyte count, anthropometric measurements, and biochemical characteristics in patients. The Spearman correlation analysis indicated that the level of Gensini’s score was significantly correlated with age (r=0.225, P=0.000), DBP (r=-0.106, P=0.017), fasting blood glucose (r=0.195, P=0.000), urea (r=0.137, P=0.002), creatinine (r=0.165, P=0.000), leukocyte count (r=0.303, P=0.000), neutrophil count (r=0.326, P=0.000), monocyte count (r=0.253, P=0.000), hemoglobin (r=-0.133, P=0.003), and erythrocyte count (r=-0.094, P=0.035), whereas a significant correlation was not found between Gensini’s score and Body Mass Index, SBP, total cholesterol, triglyceride, uric acid, eosinophil count, basophil count, lymphocyte count, or platelet count.

Full table
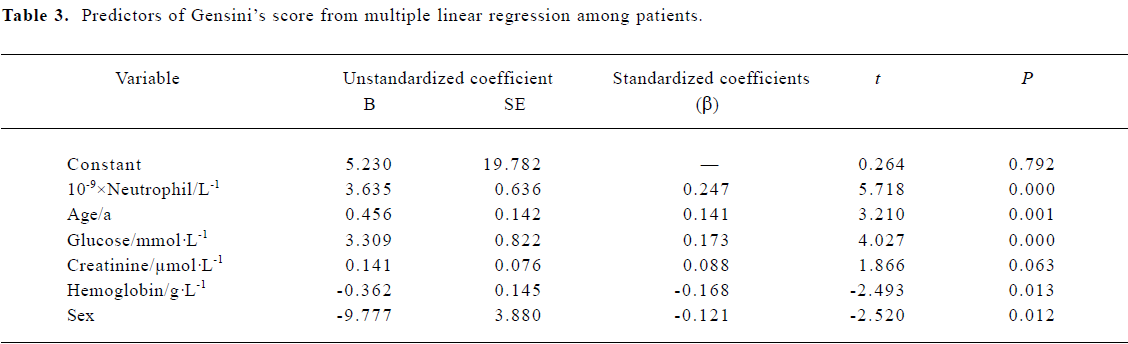
Multiple linear regression analysis with Gensini’s score as dependent variable To examine the independent associations between Gensini’s score and leukocyte count, multiple linear regression analysis was performed. In this model, Gensini’s score was used as the dependent variable and the independent variables included age, sex, smoking status, drinking status, body mass index, SBP, DBP, total cholesterol, triglyceride, fasting blood glucose, urea, creatinine, uric acid, leukocyte count, neutrophil count, eosinophil count, basophil count, lymphocyte count, hemoglobin, erythrocyte count, and platelet count. In the final model (Table 3), neutrophil count (β=0.247, P=0.000), age (β=0.141, P=0.001), glucose (β=0.173, P=0.000), creatinine (β=0.088, P=0.063), hemoglobin (β=-0.168, P=0.013) and sex (men were coded as 1 and women were coded as 2; β=-0.121, P=0.012) were significantly independently associated with Gensini’s score.
Full table
Discussion
Cardiovascular disease is the leading cause of death in the world[6]. One of its most insidious forms is coronary heart disease due to atherosclerosis[7]. Although many risk factors for coronary heart disease have been identified, they do not fully account for all cases of the disease. Thus, searches are underway for additional biological markers and especially inflammatory markers for the disease. Numerous epidemiological and clinical studies have shown leukocyte count to be an independent risk factor for coronary heart disease, a risk factor for future cardiovascular events in individuals apparently without cardiovascular disease, and a prognostic marker of future events in patients who already have cardiovascular disease[1]. Although leukocyte count appears to be an independent predictor of cardiovascular events, some of its predictive ability can be explained by its interdependence with smoking. Therefore, further studies are needed to clarify just how prominent a role leukocytes play in the pathogenesis of coronary heart disease, as well as the clinical implications. Obviously, there is a need to determine the degree to which leukocyte count is independent of smoking and other risk factors [2].
The present study was conducted to evaluate the association between the angiographical characteristics of coronary atherosclerosis and leukocyte count in patients with suspected coronary heart disease. The main finding of the present study is that the neutrophil count is significantly associated with Gensini’s score according to one-way ANOVA, the Spearman correlation, and multiple linear stepwise regression analysis in these 507 Chinese subjects. This finding is consistent with results from previous studies, in which leukocytosis has been consistently shown to be an independent risk factor for coronary heart disease regardless of disease status[2]. Furthermore, this study suggests a link between inflammatory and coronary atherosclerosis.
Our study is the first to document the independent association of neutrophil count with the angiographical characteristics of coronary atherosclerosis, which were approximated by using Gensini’s score in Chinese subjects, and which is in agreement with the results of previous studies. In a meta-analysis of 1764 cases of coronary heart disease from 7 long-term prospective studies, involving a total of 30 374 participants, the association of coronary heart disease with neutrophil count was somewhat stronger than that with other specific leucocyte components[8]. In a prospective cohort study of 55 patients with non-ST segment elevation acute coronary syndromes and angiographically documented coronary disease, acute inflammatory markers such as neutrophil count were higher among patients with multiple angiographically complex plaques than among those without[9]. The results from an immunohistochemical study on coronary artery segments suggest that neutrophil infiltration is actively associated with acute coronary events[3]. Granulocytosis affects the development of coronary atherosclerosis through multiple pathological mechanisms that mediate inflammation, cause proteolytic and oxidative damage to the endothelial cells, plug the microvasculature, induce hypercoagulability, and promote infarct expansion[2].
Moreover, another finding of this study is that age (β=0.141, P=0.001), creatinine (µmol/L; β=0.088, P=0.063), glucose (mmol/L; β=0.173, P=0.000), hemoglobin (g/L; β=-0.168, P=0.013), and sex (men were coded as 1 and women were coded as 2, β=-0.121, P=0.012) were significantly associated with Gensini’s score after adjusting for the other cardiovascular risk factors. The results of the Atherosclerosis Risk in Communities study, a community-based study of risk factors for coronary heart disease (CHD) in middle-aged people indicated that high serum creatinine was associated with almost a 3-fold risk of coronary heart disease among middle-aged people with anemia (anemia was defined as hemoglobin <130 g/L in men and <120 g/L in women), whereas no increased risk was found in people with high serum creatinine in the absence of anemia[10]. Another study found a relationship between low hemoglobin level and adverse cardiovascular outcomes in women with suspected ischemia[11]. Several investigations as well as prospective studies have shown a significant correlation between glucose metabolism and atherosclerosis in patients without diabetes, and have shown that the glycemic milieu correlates with the cardiovascular risk according to a linear model[12]. In addition, the present study demonstrated that age and being male were independent risk factors for coronary atherosclerosis, which was consistent with results from other studies[13].
A limitation of the present study is that the subjects were from one center rather than multiple centers, which may result in selective bias; however, given the large size sample of this study, it may minimize the bias. In fact, the present study is only a cross-sectional study rather than a retrospective study. And the other limitation of the study is that it provides no information regarding the cause and effect relationship between neutrophil count and coronary atherosclerosis. Although the correlation between neutrophil count and coronary atherosclerosis is significant in the present study, the clinical significance of this finding requires further investigation.
In conclusion, the independent association of neutrophil count with the angiographical characteristics of coronary atherosclerosis as approximated by Gensini’s score strongly suggests that granulocytosis may play a role in the development of coronary atherosclerosis. Thus, it may prove to be an equally informative, but less expensive and more readily available risk marker than other currently available risk factors. Further studies are required, however, to determine the implications of using the leukocyte count to predict clinical risk and outcome.
References
- Danesh J, Collins R, Appleby P, Peto R. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: meta-analyses of prospective studies. JAMA 1998;279:1477-82.
- Madjid M, Awan I, Willerson JT, Casscells SW. Leukocyte count and coronary heart disease: implications for risk assessment. J Am Coll Cardiol 2004;44:1945-56.
- Naruko T, Ueda M, Haze K, van der Wal AC, van der Loos CM, Akira Itoh A, et al. Neutrophil infiltration of culprit lesions in acute coronary syndromes. Circulation 2002;106:2894-900.
- Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol 1983;51:606.
- Judkins MP. A percutaneous transfemoral technique. Radiology 1967;89:815-21.
- American Heart Association. Heart Disease and Stroke Statistics: 2003 Update. Dallas, Texas: American Heart Association; 2002.
- Ross R. Atherosclerosis: an inflammatory disease. N Engl J Med 1999;340:115-26.
- Wheeler JG, Mussolino ME, Gillum RF, Danesh J. Associations between differential leucocyte count and incident coronary heart disease: 1764 incident cases from seven prospective studies of 30,374 individuals. Eur Heart J 2004;25:1287-92.
- Avanzas P, Arroyo-Espliguero R, Cosin-Sales J, Aldama G, Pizzi C, Quiles J, et al. Markers of inflammation and multiple complex stenoses (pancoronary plaque vulnerability) in patients with non-ST segment elevation acute coronary syndromes. Heart 2004;90:847-52.
- Jurkovitz CT, Abramson JL, Vaccarino LV, Weintraub WS, McClellan WM. Association of high serum creatinine and anemia increases the risk of coronary events: results from the prospective community-based atherosclerosis risk in communities (ARIC) study. J Am Soc Nephrol 2003;14:2919-25.
- Arant CB, Wessel TR, Olson MB. Hemoglobin level is an independent predictor for adverse cardiovascular outcomes in women undergoing evaluation for chest pain: results from the National Heart, Lung, and Blood Institute Women’s Ischemia Syndrome Evaluation Study. J Am Coll Cardiol 2004;43:2009-14.
- Sasso FC, Carbonara O, Nasti R, Campana B, Marfella R, Torella M, et al. Glucose metabolism and coronary heart disease in patients with normal glucose tolerance. JAMA 2004;291:1857-63.
- Faxon DP, Creager MA, Smith SC Jr, Pasternak RC, Olin JW, Bettmann MA, et al. Atherosclerotic vascular disease conference. Executive summary: atherosclerotic vascular disease conference proceeding for healthcare professionals from a Special Writing Group of the American Heart Association. Circulation 2004;109:2595-604.