
Thrombolytic efficacy of native recombinant staphylokinase on femoral artery thrombus of rabbits
Introduction
Staphylokinase (SAK) is an extracellular protein of 136 amino acids and is excreted by staphylococcus aureus. Its ability to dissolve thrombus was first discovered in 1948, which intrigued most scholars in the field. However, its application has not been adapted in the clinical setting due to poor purity of production and lack of natural resources. Recombinant staphylokinase (r-SAK) is a third generation thrombolytic agent produced by genetic engineering[1,2], and it has not yet been introduced to the market both in China and abroad. The r-SAK of interest in this research was created by the Shanghai Institute of Botany and Biophysiology (Shanghai, China) and was certified as the type I national new drug. This study aims to investigate the thrombolytic efficacy, ideal dosage and administration route of native r-SAK in animal experiments, which may offer basic evidence for clinical application.
Materials and methods
Study subjects Forty New Zealand male rabbits, 2.0 to 2.5 kg, were randomly assigned into 8 groups of 5 rabbits each: control, r-SAK low-dose group, medial-dose group, high-dose group, r-SAK single bolus group, allied therapy group (r-SAK+heparin), r-SK group, and the UK group.
Thrombolytic agents r-SAK freeze-dry powder was produced by the Shanghai Institute of Botany and Biophysio-logy (China) and Chengdu Jingpeng Bioengineering Co Ltd (Chengdu, Sichuan, China; batch N
Establishment of rabbit right femoral artery thrombosis model[3] The rabbit was first anesthetized with 3% pentobarbital sodium (40 mg/kg) and then fixed onto the operation table. The left femoral vein and bilateral femoral arteries were isolated and a catheter was placed into the left femoral vein for collection of blood sample. Two other catheters were placed in the femoral arteries at the distal end and then connected to a pressure monitor to record the baseline pressures of the femoral arteries. Afterwards, the catheter in the right femoral artery was removed and a balloon of (2.0–2.5 mm)×20.0 mm was inserted into the proximal part of the femoral artery. The balloon was then dilated with 8−12 atm and pushed and pulled 3 times to injure the endothelium of the femoral artery. Finally, the balloon was removed and a catheter was inserted once again for dynamically monitoring the pressure.
Thrombolytic therapy The drugs were infused through the parallel-ear vein via a pump 2 h post balloon injury as follows: the control group was given normal sodium (NS) 10 mL iv for 30 min; the r-SAK low-dose group was given r-SAK 0.25 mg/kg iv for 30 min; the r-SAK medial-dose group was given r-SAK at 0.5 mg/kg iv for 30 min; the r-SAK high-dose group was given r-SAK 1.0 mg/kg iv for 30 min; the r-SAK single bolus group was given r-SAK 0.5 mg/kg iv for 2 min; the allied therapy group was given 200 U/kg heparin, followed by an intravenous infusion of r-SAK 0.5 mg/kg for 30 min, and a subsequent infusion of heparin 50 U·kg–1·h–1 for 4.5 h; the r-SK group were given r-SK 3.0×104 U/kg iv for 30 min; and the UK group were given UK 3.0×104 U/kg iv for 30 min. The blood pressures in the rabbits’ femoral arteries were monitored consistently during the experiment for 5 h in order to evaluate the patency status of the femoral arteries described by Rebello[4].
Femoral artery angiogram Some of the rabbits received femoral artery angiogram. The selected rabbits underwent skin preparation, sterilization and local anesthesia. The right common carotid artery of the rabbit was then isolated, and a catheter was carefully introduced into the lower part of the abdominal aorta through the right common carotid artery and aortic arch. The angiogram of the bilateral femoral arteries was produced by digital subtraction angiography with a contrast medium of iopromide.
Pathological examination The balloon-injured segment of the femoral arteries was dissected 5 h subsequent to throm-bolysis. The segments were retained in 10% formaldehyde solution, imbedded in paraffin, sliced and stained by hemagglutinin-esterase. The pathological results were acquired under microscope.
Statistical analysis Data were expressed as mean±SD. Student’s t-test was used to evaluate the changes of pressures pre and post thrombolysis and the quantified variables of patency status in the different groups. Four fold table exact probability ratio was used to compare the recanalization rates in the different groups. Kruskall-Wallis test was used to analyze the nonparametric variables of the patency status post thrombolysis in each group.
Results
Changes of the pressure of left femoral artery There was no significant change of the pressure of the left femoral artery in each group after balloon injury or in the control group after NS infusion. The diastolic and mean pressures significantly decreased 75 min and 60 min post thrombolysis respectively in the r-SAK low-dose group (P<0.05). However, the systolic and pulse pressures did not change. In the r-SAK medial-dose group, the diastolic and mean pressures significantly decreased 45 min post thrombolysis (P<0.05) and the systolic pressure significantly decreased 150 min post thrombolysis (P<0.05), while the mean pressure did not change. In the r-SAK high-dose group, the diastolic and mean pressures significantly decreased 30 min and 45 min post thrombolysis respectively, and the systolic pressure significantly decreased 75 min post thrombolysis, while the pulse pressure did not change. In the r-SAK single bolus group, the systolic, diastolic and mean pressures significantly decreased 45, 70, and 30 min post thrombolysis respectively (P<0.05), and the pulse pressure did not change. In the r-SAK allied therapy group, the systolic pressure significantly decreased 120 min post thrombolysis (P<0.05), while the diastolic, mean and pulse pressures did not change. There was no significant change of the pressure of the left femoral artery in the r-SK group post thrombolysis. The diastolic and mean pressures significantly decreased 150 and 210 min respectively post thrombolysis in the UK group (P<0.05), while the systolic and pulse pressures did not change.
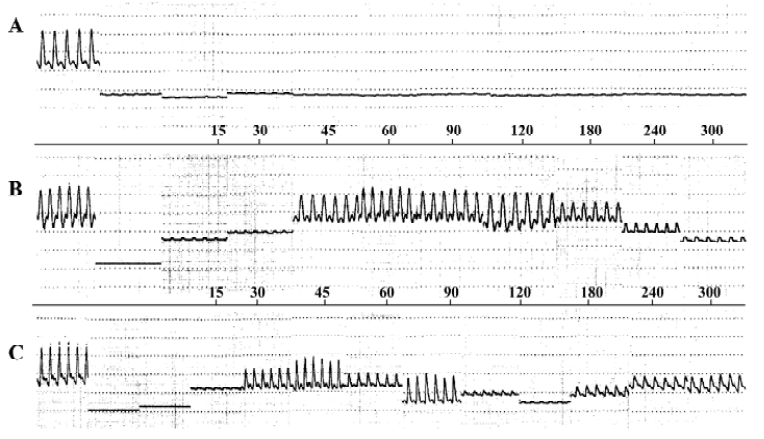
Changes of the pressure of right femoral artery The pulse, systolic, and mean pressures significantly decreased after balloon injury in the control group, while the diastolic pressure first increased and then decreased. The pulse pressure decreased to 1.0±0.7 mmHg 120 min post balloon injury in the control group, which was lower than 10% of the pulse pressure of the left femoral artery. There was no evidence of recovery after NS infusion. The pressures of the right femoral arteries in the study groups followed the same tendency of changes as in the control after balloon injury. However, some study groups displayed a peak summit in the pressure-time curve post thrombolysis with the pulse pressures reaching more than 50% of the left femoral arteries in some rabbits. The numbers are: 2 in the r-SAK low-dose group, 5 in the medial-dose group, 5 in the high-dose group, 4 in the single bolus group, 5 in the allied therapy group, and 0 in both the UK and r-SK groups. The pulse pressures of these arteries all decreased to less than 50% of the left femoral arteries 5 h post thrombolysis (Figure 1).
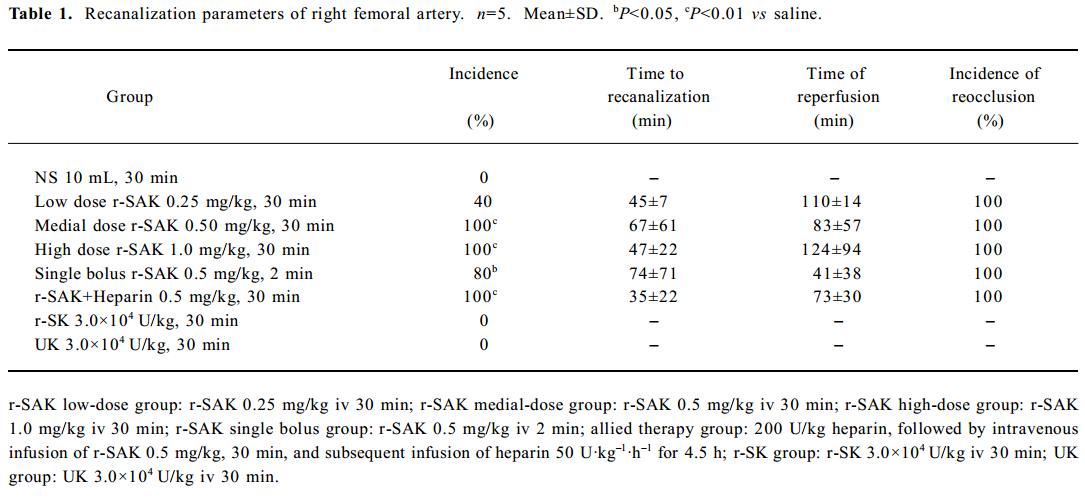
The recanalized femoral arteries after thrombolytic therapy The following is the artery reopening rate in each group: 0 in the control group, 2 in the r-SAK low-dose group, 5 in the medial-dose group, 5 in the high-dose, 4 in the single bolus, 5 in the allied therapy group, and 0 in both the UK and r-SK groups. The reopening rates in the r-SAK medial and high-dose groups (P<0.01) were significantly higher than that of the control, and there was a tendency of increasing of the reopening rate as the dosage of r-SAK given increased. The reopening rate reached 100% when the dosage exceeded 0.5 mg/kg. There was no statistical difference concerning the reopening rate, reopening time and reperfusion time among the different r-SAK dosage groups and the same dosage groups with different administration manners. The reperfusion time in the r-SAK single bolus group and the reopening time in the allied therapy group had a tendency to be shorter. The reopening rate was significantly higher in the r-SAK group than in both the r-SK and UK groups administered with the corresponding dosage. All the recanalized arteries reoccluded at the end of the study (Table 1; Figure 2).
Full table
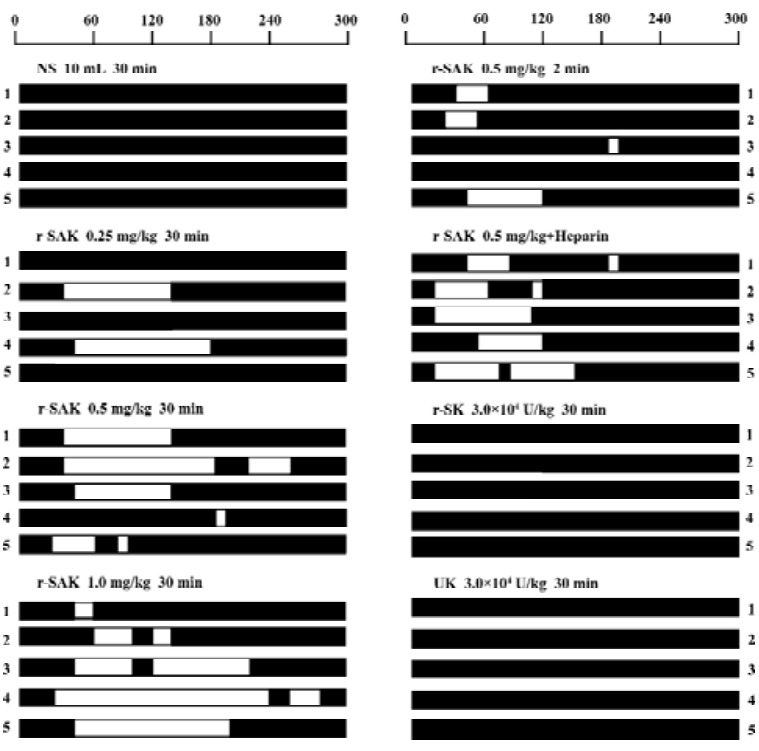
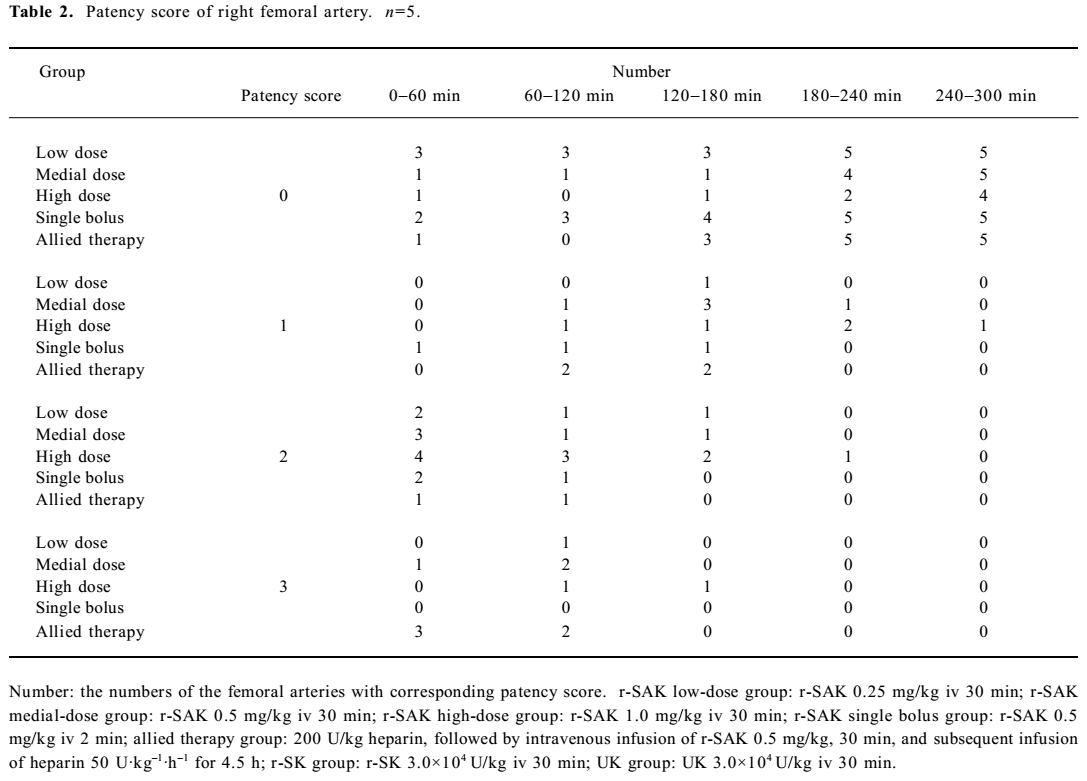
Patency status of right femoral arteries post thrombolysis The patency status of the right femoral arteries were classified quantitatively according to pulse pressures in reference to studies published by Rebello[4] and Collen[5]. Statistical analysis showed that the patency status in the different r-SAK dosage groups had no differences during each time period, but the ranks in both the r-SAK medial and high-dose groups were higher than that in the low dose group (all P<0.01), and there was no significant difference between the medial and high-dose groups (P=0.053). There were also no differences in the patency status of the right femoral arteries among the groups which received the same dosage of r-SAK, but administered in different manners, while the ranks of the patency status during each period were significantly higher in the r-SAK infusion and allied therapy groups than that in the single bolus group (P<0.01 and P<0.05, respectively), and there was no difference between the r-SAK infusion group and the allied therapy group (P=0.60; Table 2).
Full table
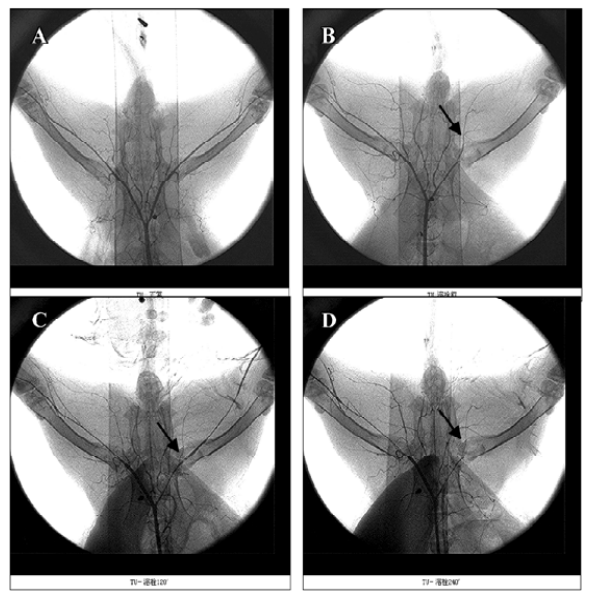
Angiogram of the femoral artery An angiogram showed that the rabbits’ femoral arteries were undamaged with fluent blood flow originally. The right femoral arteries were totally occluded within 120 min after balloon injury which indicated that occlusive thrombus formed at the site. Some arteries were reopened after r-SAK thrombolysis, but all the reopened arteries were reoccluded at the end of the experiment (Figure 3).
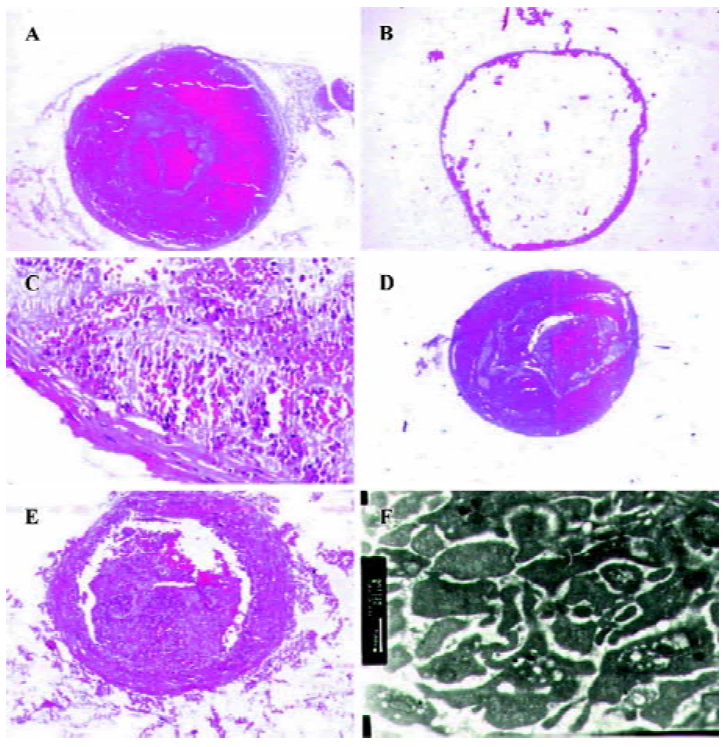
Pathology of the artery A pathological test showed that the femoral arteries were totally occluded 120 min after balloon injury (Figure 4A), and some of the arteries were reopened after r-SAK thrombolysis (Figure 4B). A pathological slice from the unopened artery in the single bolus group showed that the undissolved thrombus was enriched with degenerated platelets and neutrophils (Figure 4C). The slices from the UK and r-SK groups after thrombolysis showed that the lumen was filled with degenerated platelets, neutrophils and erythrocytes, which formed the mixed thrombus (Figure 4D). All the recanalized arteries reoccluded 5 h post thrombolysis and the re-formed thrombus contained mainly degenerated platelets and neutrophils (Figure 4E, 4F).
Discussion
r-SAK is a new type, third generation thrombolytic agent, which was first produced by genetic engineering in 1985[1,2]. Some studies showed that r-SAK induced early, complete, and sustained coronary artery patency at least as frequently as the accelerated recombinant tissue type plasminogen activator without associated fibrinogen degradation[6,7]. Native r-SAK was created by the Shanghai Institute of Botany and Biophysiology (China) in 1990, which is a molecular cloning of the SAK gene in Escherichia coli, and is highly purified and crystallized in white color freeze-dry powder with biological characteristics very similar to natural SAK[8]. It has recently been certified as the type I national new drug. Yet its efficacy has not been fully evaluated both experimentally and clinically. Therefore, this study aims to investigate the thrombolytic efficacy, ideal dosage and administration of native r-SAK through animal experimentation, which may offer basic evidence for clinical use.
The purposes of observing the pressure of the left femoral artery are: (1) to act as a control for the pressure of the right femoral artery; and (2) to observe the effect of native r-SAK on systemic blood pressure. As a result, the pressure of the left femoral artery in each r-SAK dosage group decreased significantly. This may be due to the following factors: (1) capillary hemorrhage occurred in the field surrounding the procedure post thrombolysis, which may lead to hypovolemia and decreased blood pressure; (2) many blood samples were collected for tests and there was a lack of transfusion and nourishment given to the subjects; and (3) native r-SAK caused the decrease of the blood pressure directly. The decrease of blood pressure did not threaten the lives of the animals and all the rabbits were kept alive until the end of each experiment.
The pressure of the right femoral artery in each group decreased significantly post balloon injury and the pulse pressure decreased to 0 or less than 10% of the left femoral artery. This indicated that the thrombus had formed and the lumen of the artery was occluded[4]. The pulse pressures of the right femoral arteries did not change in the control group after NS infusion, which indicated that the arteries were still occluded. However, the pulse pressures returned to the baseline status or more than 50% of the left femoral arteries in some of the animals in the study groups, and the systolic, diastolic and mean pressures were all enhanced significantly, which indicated that the thrombus was dissolved and the arteries reopened. There was no difference among the different r-SAK dosage groups concerning the reopening rate, the time to reopening and the reperfusion time. The recanalization rate had a tendency to increase as the r-SAK dosage increased, and it reached 100% as the dosage administered exceeded 0.5 mg/kg. The patency status of the recanalized arteries in the different dosage groups had no difference during each period, but the ranks in both the r-SAK medial and high-dose groups were higher than that in the low-dose group (all P<0.01), which indicated that the patency status may improve as the dosage given increased. The recanalization rate reached 80% in the r-SAK single bolus group, which was significantly higher than that of the control. However, concerning the time to reopening, the reopening rate, the reperfusion time and the patency status post thrombolysis, the administration manner of single bolus did not show any superiority to infusion. The reopening rate reached 100% and the time to reopening displayed a tendency to be shorter in the r-SAK allied therapy group, in addition, the reperfusion time had no difference compared with the other groups, which may be due to a smaller sample size of subjects.
This study showed that the reopening rate of r-SAK was significantly higher than that of r-SK and UK when administered at the same dosage. After thrombolysis by r-SK, the systolic, diastolic and mean pressures of the right femoral arteries temporarily increased, but the pulse pressure did not change. This indicated that the thrombus might be partially dissolved, but the arteries did not reopen in the end due to weaker potency of r-SK. The pressures of the right femoral arteries did not change post thrombolysis in the UK group, which indicated that the thrombolytic potency of UK might be even less than that of r-SK.
A specific phenomenon of the pressure waves was found in this experiment, which showed that the pulse pressure of the right femoral arteries changed in a fluctuant manner (Figure 1). This phenomenon may be due to the creation of a local hypercoagulable state produced by the release of various procoagulate factors of the thrombus dissolution. This may contribute to the reformation of the thrombus and lead to the deterioration of blood flow. Thrombus formation and dissolution is inversely related and one may increase as the other decreases. This can contribute to the constant alteration of the lumen of the artery and account for the fluctuant manner of the pulse pressure. The pulse pressures of right femoral arteries in all the reopened vessels decreased to 0 or less than 50% of the left femoral arteries 5 h post thrombolysis, which indicated that the thrombus reformed in the lumens and the arteries became stenotic or reoccluded. This may be due to following reasons: (1) the balloon created a deep injury of the femoral artery, which increased the likelihood of thrombus formation[9]; (2) the catheter blocked the distal part of the artery, and this might have promoted thrombus formation; and (3) anti-platelet drugs were not used in the experiment.
Pathological testing of the reformed thrombus showed that it was enriched with degraded platelets and neutrophils, which indicated that the platelet played a very important role in the mechanism of thrombus reformation. Similar to other fibrin select thrombolytic agents, r-SAK allied therapy with anti-platelet and anticoagulant drugs may be a necessary way for avoiding thrombus reformation post thrombolysis.
In conclusion, native r-SAK has a definite thrombolytic effect on the femoral artery thrombus of rabbit. The recanalization rate reached 100% as the dosage amount exceeding 0.5 mg/kg. Single bolus r-SAK is an effective administration manner, which may be used in emergent status such as pre-hospital thrombolysis. r-SAK allied therapy with the addition of heparin may improve the thrombolytic results in terms of shortening the time to recanalization. The thrombolytic efficacy of native r-SAK is superior to that of r-SK and UK when administered at the same dosage.
Acknowledgements
We thank Mr Guo-ping YANG (Animal Experiment Center, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China) for his assistance in animal experiment and Prof Zheng-qing FENG (Department of Pathology, Nanjing Medical University, Nanjing, China) for his assistance of pathological examination.
References
- Toombs CF. New directions in thrombolytic therapy. Curr Opin Pharmacol 2001;1:164-8.
- Szemraj J, Walkowiak B, Kawecka I, Janiszewska G, Buczko W, Bartkowiak J, et al. A new recombinant thrombolytic and antithrombotic agent with higher fibrin affinity-a staphylokinase variant. I. In vitro study. J Thromb Haemost 2005;3:2156-65.
- Li CJ, Huang J, Yang GP, Xu YN, Lu L, Feng ZQ. An animal model of the femoral artery thrombosis in rabbit by balloon injury. Acta Univ Med Nanjing 2001;21:277-80.
- Rebello SS, Driscoll EM, Lucchesi BR. TP-9201, a glycoprotein IIb/IIIa platelet receptor antagonist, prevents rethrombosis after successful arterial thrombolysis in the dog. Stroke 1997;28:1789-96.
- Collen D, Cock FD, Stassen FM. Comparative immunogenicity and thrombolytic properties toward arterial and venous thrombi of streptokinase and recombinant staphylokinase in baboons. Circulation 1993;87:996-1006.
- Vanderschueren S, Barrios L, Kerdsinchai P, De Man F, Muyldermans L, Collen D, et al. A randomized trial of recombinant staphylokinase versus alteplase for coronary artery patency in acute myocardial infarction. The STAR Trial Group. Circulation 1995;92:2044-9.
- Vanderschueren S, Dens J, Kerdsinchai P, Desmet W, Vrolix M, De Man F, et al. Randomized coronary patency trial of double-bolus recombinant staphylokinase versus front-loaded alteplase in acute myocardial infarction. Am Heart J 1997;134:213-9.
- Tang QQ, Zhang XX, Yu M, Song HY. Isolation, purification and crystallization of recombinant staphylokinase (r-Sak). Pharm Biotech 1997;4:1-4.
- Merhi Y, Guidoin R, Provost P, Leung TK, Lam JY. Increase of neutrophil adhesion and vasoconstriction with platelet deposition after deep arterial injury by angioplasty. Am Heart J 1995;129:445-51.